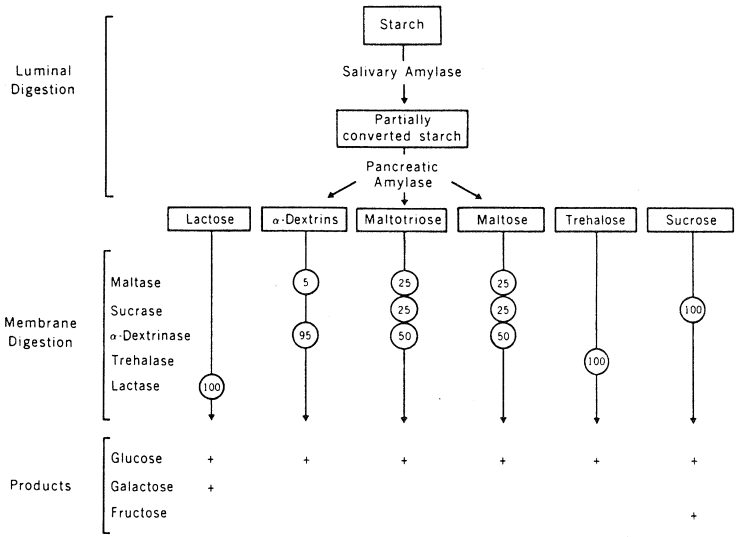
Plant starch is the main dietary carbohydrate, being composed of glucose units held together by 1,4-α-glycosidic linkages with 1,6-α-glycosidic branch points. Starch is hydrolyzed by salivary and pancreatic amylases with subsequent hydrolysis of maltose and limit dextrins by a limited number of enzymes such as maltase and a-dextrinase which are intrinsic membrane proteins of the epithelial cells of the brush border of the intestinal mucosa.
These enzymes are freely accessible from the lumen and are located in close proximity to active transport sites. Enzyme concentrations are highest in the mid-jejunum and upper ileum where ingested maltose and sucrose are also digested by equivalent processes. Maltase, α-dextrinase and sucrase are components of the sucrase-isomaltase complex and, on contact with these brush border enzymes, substrate saccharides are hydrolyzed to release products that are available for absorption. Lactase, another brush border enzyme, can hydrolyze several glycosides, the main one being lactose.
Glucose and galactose at low concentrations enter the enterocytes rapidly by means of a common sodium-dependent, energy-requiring carrier mechanism. However, when the luminal sugar concentration is high, absorption may be almost entirely passive. Passive absorption of these sugars occurs by solvent drag with water absorption, but in the absence of water movement sugars only move down a concentration gradient and then at a rate proportional to the magnitude of the gradient. Some 10% or more of the absorbed glucose may be metabolized within the absorptive cells but the remainder makes its exit from the cytosol into the intracellular space partly by diffusion but mostly via a sodium-independent carrier located at the basolateral membrane (Johnson, 1991).
Fructose is also exceptionally well absorbed but in this case by facilitated diffusion only, because, unlike the glucose-galactose carrier, the fructose carrier cannot be energized for active transport. Some control over the rate of sugar absorption is possible because stomach motility and emptying can be slowed in response to negative feedback signals from the duodenum and proximal jejunum; nevertheless, both glucose and fructose may remain transiently in the luminal contents. Although these molecules are osmotically active, the speed with which they are absorbed normally ensures that water is not required to bring the intestinal contents to isotonicity and thus osmotic diarrhoea does not occur. The capacity of the human small intestine to absorb free sugars is indeed enormous and it has been estimated that hexoses equivalent to 22 pounds of sucrose could be absorbed daily! (Johnson, 1991).
The concentration of disaccharidases can increase in response to certain changes in the diet, sucrase being inducible by an increase in dietary sucrose although lactose, galactose, and maltose do not appear to stimulate similar effects. However, disaccharidase deficiencies are known to occur, being associated with well-documented malabsorption syndromes. Lactose intolerance, which may be due to congenital or later acquired deficiency of lactase, is associated with colonic fermentation of unhydrolyzed lactose with accompanying flatulence, abdominal cramps, and the passage of lactose, lactic acid, and fatty acids in the stools. Diarrhoea occurs because of the high osmotic pressure of the colonic contents and the stimulation of peristalsis by acid products of fermentation. Rarely, deficiencies of sucrase and a-dextrinase may occur in children but maltose intolerance appears not to occur because of the existence of several enzymes capable of hydrolyzing maltose. Intolerance of glucose and galactose does occur in rare instances, apparently due to the absence of the glucose carrier and patients may be helped to recover by feeding them only fructose, whereupon symptoms disappear.
The ingestion of poorly absorbed carbohydrates leads to the development of a symptom complex of which diarrhoea is the main feature (Menzies, 1983). Diarrhoea may be defined as a stool volume greater than 500 cm3/day and is usually accompanied by increased frequency of stool passage as well as by an increased fluidity of the motions. Although the colon has a tremendous ability to absorb water, diarrhoea may occur if it is overwhelmed by the volume of fluid delivered from the small intestine or if the ileum delivers unabsorbed sugars which are osmotically active, thus reducing the absorptive capacity of the colon. In fact very few naturally occurring foods contain a high enough concentration of unabsorbable sugar to cause diarrhoea although other symptoms such as bloating, colic and flatulence may occur.